


Do you know the crucial distinctions between Crohn’s and Ulcerative Colitis? Understanding these differences can transform your approach to treatment and daily management. Let’s uncover the facts your doctor might have overlooked, so you can take control of your health with confidence and clarity.
Crohn’s disease and ulcerative colitis are the two most common types of inflammatory bowel disease (IBD), but they are far from identical. Recognizing their subtle—and sometimes profound—differences is essential for anyone living with these chronic conditions, their loved ones, or anyone seeking to better manage symptoms and long-term wellness.
This in-depth guide dives into the five key differences that matter most and shares practical, expert-driven strategies for diagnosis, management, and hope for the future of digestive health.
Understanding Inflammatory Bowel Disease: Setting the Stage
Inflammatory bowel disease (IBD) refers to a group of chronic conditions where your body’s own immune system attacks the digestive tract, causing inflammation. The two primary types are Crohn's disease and ulcerative colitis, both impacting millions of people worldwide.
While the terms are often used interchangeably, they are distinct entities with different areas of the gastrointestinal (GI) tract affected, varying symptoms, and diverse treatment approaches. Developing a solid understanding of IBD sets the foundation for better identifying what are the differences between Crohn's and ulcerative colitis.
For many, an IBD diagnosis marks the start of a lifelong health journey. Early detection, accurate diagnosis, and clear information can vastly improve quality of life. Whether you’re newly diagnosed, seeking to better manage symptoms, or supporting someone with IBD, this guide arms you with medical facts and actionable advice to partner actively with your care provider. Let’s dive into the essentials that inform, empower, and enable you to take charge of your digestive health.
The 5 key differences between Crohn's and ulcerative colitis
How inflammatory bowel disease is diagnosed
Real-life expert perspectives on management
Practical strategies for symptom relief
Overview of Crohn's Disease and Ulcerative Colitis
When people talk about bowel disease, Crohn's and ulcerative colitis are the names you’re most likely to hear. These conditions fall under the umbrella term "inflammatory bowel disease," but they each have their own triggers, disease patterns, and ways of showing up in daily life. Understanding the underlying mechanisms and distinctions between the two is the first step to a more targeted treatment plan and symptom control.
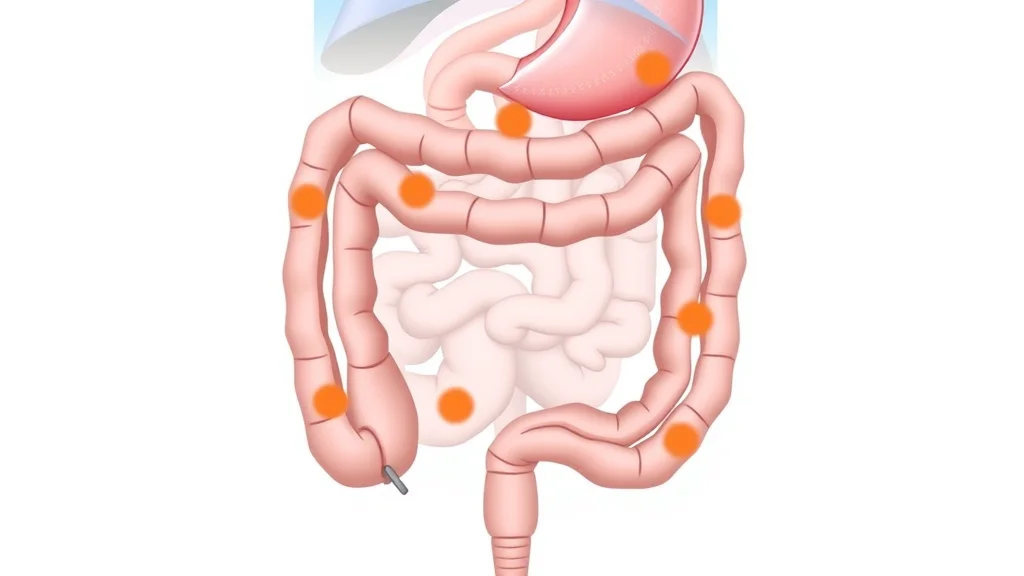
Crohn's disease can affect any part of the digestive tract, from mouth to anus, leading to patchy, irregularly scattered areas of inflammation. Ulcerative colitis, on the other hand, is limited strictly to the colon and rectum, with inflammation that’s continuous along the affected section. While both stem from immune system dysfunction and can cause significant discomfort or disruption, knowing what are the differences between Crohn's and ulcerative colitis is essential for tailored care.
Defining Crohn's Disease: Key Features
Crohn's disease is defined by its ability to affect any part of the GI tract, most commonly the small intestine, though it can also involve the colon and even other sections of the digestive system. The hallmark of Crohn’s is "transmural" inflammation—meaning the inflamed area spans through all layers of the bowel wall. This makes Crohn's disease more likely to cause complications like fistulas, strictures, abscesses, and nutrient malabsorption.
Common symptoms include abdominal pain, persistent diarrhea (sometimes with blood), unintentional weight loss, and fatigue. Some patients with Crohn’s may experience issues outside the digestive tract, such as skin rashes, eye inflammation, or joint pain, reflecting the widespread effects of this immune-driven disease. Crohn’s may flare unpredictably, requiring ongoing monitoring and a flexible, responsive treatment strategy.
Defining Ulcerative Colitis: Key Features
In contrast, ulcerative colitis is strictly confined to the large intestine (colon) and rectum. It involves only the innermost lining (the mucosa) of the colon, resulting in a pattern of continuous, superficial inflammation. Unlike the patchy presentation seen in Crohn's, the affected segment in ulcerative colitis is unbroken and extends from the rectum upwards.
The most characteristic symptoms of ulcerative colitis are bloody diarrhea, an urgent need to have bowel movements, abdominal cramps, and sometimes unexplained weight loss. Complications can include severe bleeding, toxic megacolon, and a higher risk of colon cancer over time if inflammation remains unchecked. Because the inflammation doesn’t reach the deeper layers of the bowel wall, certain complications are less common than in Crohn’s, but the potential for escalation remains significant if untreated.
What Are the Differences Between Crohn's and Ulcerative Colitis? A Side-by-Side Comparison
Feature |
Crohn's Disease |
Ulcerative Colitis |
|---|---|---|
Area Affected |
Any part of GI tract |
Colon and rectum only |
Inflammation Depth |
Transmural (full thickness) |
Mucosal (surface layer) |
Symptoms |
Abdominal pain, weight loss, diarrhea |
Bloody diarrhea, urgency |
Risk Factors |
Smoking increases risk |
Smoking may reduce risk |
Surgical Outcomes |
Recurrence likely after surgery |
Surgery often curative |
5 Key Differences: What Are the Differences Between Crohn's and Ulcerative Colitis?
Grasping what are the differences between Crohn’s and ulcerative colitis improves everything from early symptom recognition to managing flare-ups and making informed choices about treatment. Let’s break down the five crucial differences that stand out in medical research, clinical practice, and daily life for patients with these inflammatory bowel diseases.
Recognizing the unique patterns of each condition—from the specific sections of the digestive system they target, to the depth and character of inflammation—shapes your journey from uncertainty to informed, empowered living. These insights, combined with real expert perspectives and patient experiences, equip you to advocate for more effective care and long-term wellness.
1. Location: Bowel Disease Patterns in Crohn’s vs. Ulcerative Colitis
The first key difference is location within the digestive tract. Crohn’s disease can involve any segment from the mouth to the anus, though it most frequently targets the small intestine and the first part of the colon. Its patchy nature means segments of healthy tissue can exist between areas of inflammation. In contrast, ulcerative colitis is always limited to the colon and rectum, beginning at the rectum and moving upward in a continuous fashion. The large intestine’s surface layer is the only part affected.
This distinction helps explain varying symptoms and complications. For instance, Crohn’s in the small intestine may lead to malabsorption of nutrients and vitamin deficiencies, while ulcerative colitis is less likely to interfere with nutrient absorption but more likely to produce visible blood in stool. Knowing these unique bowel disease patterns is vital not just for diagnosis, but for understanding the potential impact on your daily quality of life.

2. Inflammation: Depth and Appearance in Inflammatory Bowel Disease
Inflammation in Crohn’s disease versus ulcerative colitis goes beyond location—it also varies in depth. Crohn’s inflammation is transmural, meaning it penetrates the entire thickness of the bowel wall. This full-thickness involvement makes Crohn’s more vulnerable to complications like fistulas (abnormal connections), strictures (narrowing), and deep ulcers, which can affect the surrounding tissues or organs.
Ulcerative colitis, by contrast, is limited to the mucosal layer—the surface lining of the colon. This mucosal involvement often translates to more superficial symptoms, such as bleeding and urgency, but with a lower risk of deep-seated complications. Endoscopic exams and biopsies play a critical role in distinguishing between these two conditions by revealing these characteristic patterns, which are crucial to selecting the safest and most effective treatment plan for each patient.
It's also worth noting that some autoimmune conditions, such as scleroderma, can present with overlapping gastrointestinal symptoms and may complicate the diagnostic process for IBD. If you're interested in understanding how scleroderma symptoms and management compare to those of Crohn’s and ulcerative colitis, you can find a comprehensive overview in our guide to scleroderma symptoms and management.
3. Symptoms: How Disease or Ulcerative Colitis Manifests in Daily Life
Crohn’s and ulcerative colitis can both be disruptive but produce somewhat different everyday hardships. With Crohn’s, symptoms often include abdominal pain (often on the right side or around the navel), ongoing diarrhea, unintentional weight loss, and sometimes nausea or mouth ulcers. Flare-ups may also lead to fevers, night sweats, and even issues outside the GI tract, such as eye or skin inflammation.
Ulcerative colitis, meanwhile, tends to present as frequent, urgent, and often bloody diarrhea, lower abdominal pain, and sometimes tenesmus (the sensation of needing to have a bowel movement even when the colon is empty). Because it is confined to the colon, nutritional absorption issues are less prominent but the emotional burden can be substantial due to the social inconvenience and anxiety that frequent, urgent trips to the bathroom entail. Recognizing these patterns helps people with IBD navigate daily life, communicate symptoms accurately, and manage symptoms proactively.

4. Complications: Risk Profiles for Each Inflammatory Bowel Condition
Complications add another layer of distinction between the two main types of inflammatory bowel disease. Crohn’s disease carries a higher risk for issues like bowel obstructions, deep tissue infections, and fistulas, primarily because of the transmural nature of its inflammation. Over time, the affected parts of the digestive tract can become scarred or narrowed, leading to recurring symptoms or emergency situations that may require surgical intervention.
Ulcerative colitis, on the other hand, is less likely to result in strictures or fistulas, but does present a heightened long-term risk of colon cancer and severe acute episodes like toxic megacolon. Routine screening and surveillance are recommended for patients with longstanding ulcerative colitis to monitor for dysplasia or early changes indicating a progression toward cancer. Balancing vigilance with symptom management is vital for reducing risks on both fronts.
5. Treatments: Medical vs. Surgical Approaches in Disease and Ulcerative Colitis
Treatment strategies recognize and adapt to the structural and functional differences between Crohn’s and ulcerative colitis. Most patients begin with medications that reduce inflammation or modulate the immune system, such as aminosalicylates, corticosteroids, immunomodulators, or biologics. However, Crohn’s disease is notorious for recurring in previously unaffected segments, even after surgical removal of the diseased area, making lifelong medical management essential in many cases.
Ulcerative colitis, by comparison, can be permanently “cured” in some cases with surgical removal of the colon (proctocolectomy), which virtually eliminates the risk for future colonic disease. Nonetheless, this is a major surgery with its own set of adaptations and potential complications. Personalized treatment plans, frequent checkups with a care professional, and ongoing education are core components of managing either disease and ulcerative colitis for the best possible outcomes.
“Recognizing the distinctions between Crohn’s and ulcerative colitis can empower patients to advocate for the most effective care options.” — Dr. Leslie Carr, Gastroenterologist, Cleveland Clinic
Indeterminate Colitis: When Diagnosis Isn’t Clear
About 10% of people with inflammatory bowel disease are initially diagnosed with indeterminate colitis, a form where the clinical, endoscopic, and even histological features overlap between Crohn’s disease and ulcerative colitis. This can make establishing an effective treatment plan challenging in the early stages. For these individuals, careful monitoring and repeated evaluation are essential, as the true nature of the bowel disease may only clarify over time with new symptoms or evolving diagnostic signs.
Since management relies so heavily on an accurate diagnosis, patients with indeterminate colitis often require a broader treatment approach that is flexible enough to adapt as more information becomes available. Ongoing collaboration with skilled care professionals ensures that neither symptoms nor potential complications are overlooked, no matter where on the spectrum of inflammatory bowel diseases a person falls.
“Around 10% of patients initially receive a diagnosis of indeterminate colitis, where the features of both diseases overlap.” — Dr. Martin Evans, Inflammatory Bowel Specialist
How Doctors Diagnose: The Role of Imaging and Lab Tests in Inflammatory Bowel Disease
Diagnosis of Crohn’s disease and ulcerative colitis relies on a combination of clinical evaluation, blood cell analysis, stool studies, advanced imaging, and endoscopic examination. Common tools include colonoscopy (visualizing the colon and obtaining biopsies), CT or MRI enterography (to assess the small intestine, deep lesions, and complications), and laboratory markers identifying inflammation.
These tests not only distinguish between Crohn’s and ulcerative colitis by showing the area and depth of the inflamed region, but also help rule out infections or other conditions that can mimic symptoms. Imaging is especially useful for detecting disease in harder-to-reach areas of the digestive system, and for forming a complete picture of disease activity and extent. Early, accurate diagnosis leads to a more targeted, effective treatment plan tailored to the unique needs of each patient.

“Imaging and endoscopy help us pinpoint the exact nature of each patient’s inflammatory bowel disease, contributing to a more personalized treatment plan.” — Dr. Natasha Green, Colorectal Surgeon
Living With Inflammatory Bowel Disease: Patient Perspectives
For many people with IBD, the journey doesn’t end after diagnosis. Daily life means learning how to manage symptoms, reduce triggers, and protect long-term gut health. Practical lifestyle adjustments, emotional resilience, and community support all play critical roles in ensuring quality of life. Whether living with Crohn’s disease or ulcerative colitis, partnering with your care professional is key.
Building a flexible and responsive support network, staying up-to-date with new research, and committing to regular health check-ins empower people with IBD to move forward with hope and adaptive strategies. Remember, each person’s experience is unique, so what works for one may not work for another—but you’re never alone in the journey.
Dietary adjustments
Stress reduction strategies
Medication adherence
Community support resources
Expert Recommendations: Evidence-Based Strategies for Symptom Management
Modern treatment for Crohn’s and ulcerative colitis is guided by ongoing research, patient preferences, and clinical expertise. Evidence-based strategies include early use of biologic medications to reduce inflammation, personalized nutritional plans, monitoring of disease activity, and timely adjustment of medications to reduce the risk of serious complications or surgery. Quit smoking, as it increases risk in Crohn’s, but sometimes is discussed as a risk-modifier in ulcerative colitis.
Working closely with your healthcare team, including gastroenterologists, dietitians, mental health professionals, and community resources, is central to optimal disease control and quality of life. Open dialogue, shared decision-making, and evidence-based knowledge are your strongest allies in navigating inflammatory bowel disease, ensuring the most effective, least disruptive treatment options are always front and center.
Latest Guidelines on Disease and Ulcerative Colitis Treatments
The most up-to-date guidelines recommend a stepwise approach, beginning with medications like aminosalicylates and steroids for mild to moderate disease, and progressing to immunomodulators or biologic therapies for severe, persistent cases. For patients with complications, surgical intervention remains vital. Regular monitoring for bone health, cancer screening, and vaccine updates are part of comprehensive long-term management. Ultimately, what are the differences between Crohn's and ulcerative colitis often dictate the treatment paths and follow-up needed for each patient.
Alongside conventional medicine, emerging therapies and research into personalized, precision medicine hold promise for making the chronic journey of inflammatory bowel disease more manageable and less disruptive, now and in the future.
Key Takeaways: What Are the Differences Between Crohn's and Ulcerative Colitis?
Location: Crohn’s can affect any part of the GI tract in a patchy pattern, while ulcerative colitis remains limited to the colon and rectum, with continuous involvement. Inflammation Depth: Crohn’s inflammation penetrates all layers of the bowel wall; ulcerative colitis affects only the surface lining.
Symptoms: Crohn’s presents with abdominal pain, diarrhea, and weight loss; ulcerative colitis with bloody diarrhea and urgency. Complication Risks: Crohn’s is prone to strictures, fistulas; ulcerative colitis increases risk of colon cancer. Treatment Outcomes: Crohn’s may recur post-surgery; ulcerative colitis can be cured with colon removal.
Frequently Asked Questions: What Are the Differences Between Crohn's and Ulcerative Colitis?
Which is more serious, Crohn's or ulcerative colitis?
Both Crohn’s and ulcerative colitis can be serious, but Crohn’s tends to have a broader range of complications due to its ability to affect the entire gastrointestinal tract and deeper tissue layers. However, ulcerative colitis may increase risk for colon cancer if left untreated. Severity truly depends on individual disease course and response to treatment.
Can Crohn's cause nosebleeds?
While Crohn's primarily affects the digestive tract, its complications (like nutritional deficiencies or side effects from medications) can make some patients more prone to nosebleeds. However, nosebleeds are not a classic hallmark of the disease.
How to differentiate Crohn's disease and ulcerative colitis?
Differentiation is based on endoscopic findings, biopsy results, the specific location and depth of inflammation, and associated symptoms. Crohn’s has patchy, deep inflammation and can affect any part of the gut, while ulcerative colitis is continuous and limited to the colon’s inner lining.
Conclusion: Empowering Your Health Journey—Crohn's and Ulcerative Colitis Management
Understanding the key differences between Crohn’s and ulcerative colitis allows you and your care team to choose the right tools, strategies, and support—empowering you to live fully and well.
Explore More—Your Path to Better Wellness Continues
As you continue to build your knowledge about inflammatory bowel disease, you may find it helpful to explore how other chronic conditions intersect with gut health and overall wellness. For a broader perspective on resilience, hope, and navigating complex health journeys, discover the inspiring story of a young cancer survivor’s path to remission and renewed strength in our feature on hope and resilience after cancer. Expanding your understanding can empower you to approach your own health with greater confidence and optimism.
Sources
Crohn's & Colitis Foundation – https://www.crohnscolitisfoundation.org/
MedlinePlus: Crohn's Disease – https://medlineplus.gov/crohnsdisease.html
MedlinePlus: Ulcerative Colitis – https://medlineplus.gov/ulcerativecolitis.html
Mayo Clinic: Ulcerative Colitis – https://www.mayoclinic.org/diseases-conditions/ulcerative-colitis/
NHS: Ulcerative Colitis – https://www.nhs.uk/conditions/ulcerative-colitis/
NHS: Crohn's Disease – https://www.nhs.uk/conditions/crohns-disease/
Understanding the distinctions between Crohn’s disease and ulcerative colitis is crucial for effective diagnosis and management. Both are forms of inflammatory bowel disease (IBD) but differ in several key aspects: Location of Inflammation: Crohn’s disease can affect any part of the gastrointestinal tract, from the mouth to the anus, often in a patchy distribution. In contrast, ulcerative colitis is confined to the colon and rectum, with continuous inflammation starting from the rectum and extending proximally. (mayoclinic. org)
Depth of Inflammation: In Crohn’s disease, inflammation can penetrate all layers of the bowel wall (transmural), leading to complications like strictures and fistulas. Ulcerative colitis involves only the innermost lining (mucosa) of the colon, resulting in superficial inflammation. (mayoclinic. org)
Pattern of Inflammation: Crohn’s disease often presents with “skip lesions,” where inflamed areas are interspersed with healthy tissue. Ulcerative colitis, however, exhibits a continuous pattern of inflammation without healthy segments in between. (mayoclinic. org)
Symptoms: Both conditions can cause abdominal pain and diarrhea. However, ulcerative colitis is more likely to result in bloody diarrhea and an urgent need to defecate, while Crohn’s disease may lead to weight loss and malnutrition due to its impact on nutrient absorption. (mayoclinic. org)
Complications and Surgical Outcomes: Crohn’s disease carries a higher risk of complications such as fistulas and strictures, and surgery may not cure the disease as it can recur in other areas of the GI tract. In contrast, surgical removal of the colon and rectum in ulcerative colitis can be curative. (mayoclinic. org)
For a more detailed comparison, you can refer to the Mayo Clinic’s comprehensive overview on the differences between ulcerative colitis and Crohn’s disease. (mayoclinic. org) Additionally, the Crohn’s & Colitis Foundation provides an informative guide that delves into the distinctions between these two conditions. (crohnscolitisfoundation. org)
If you’re seeking a visual explanation, the following video offers a concise summary of the key differences between ulcerative colitis and Crohn’s disease: Ulcerative colitis vs. Crohn’s disease









Write A Comment